
- The bladder is not sterile! (1)
- Many of us were taught that the bladder is a sterile environment but this is not the case. There is a urobiome with commonly found organisms that live in the bladder.
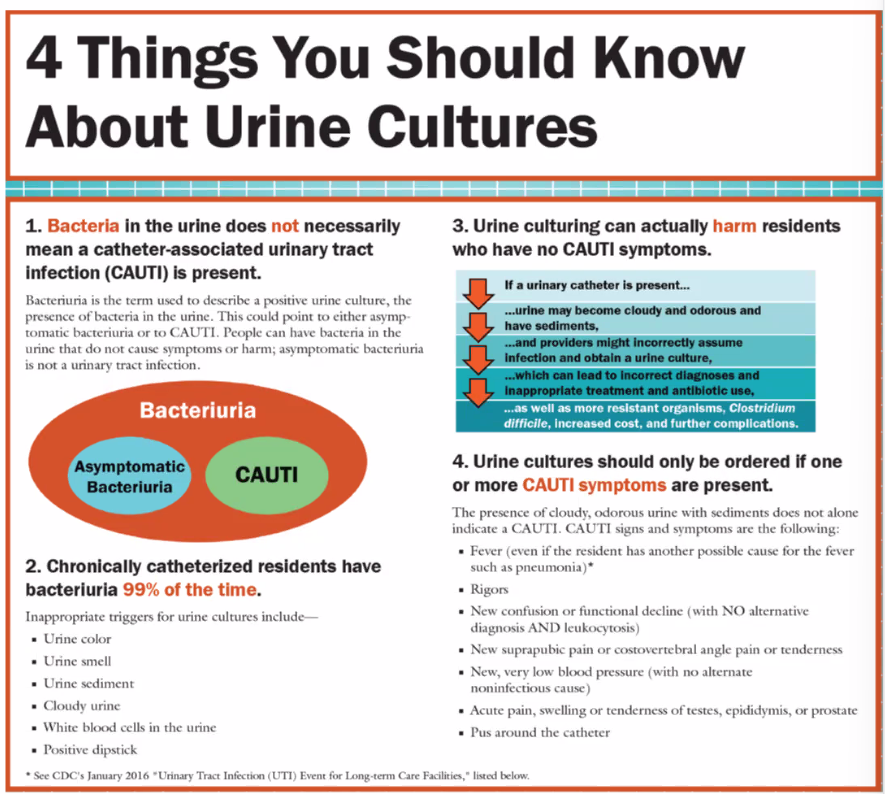
- About 50% of those in LTC will have asymptomatic bacteriuria. (2)
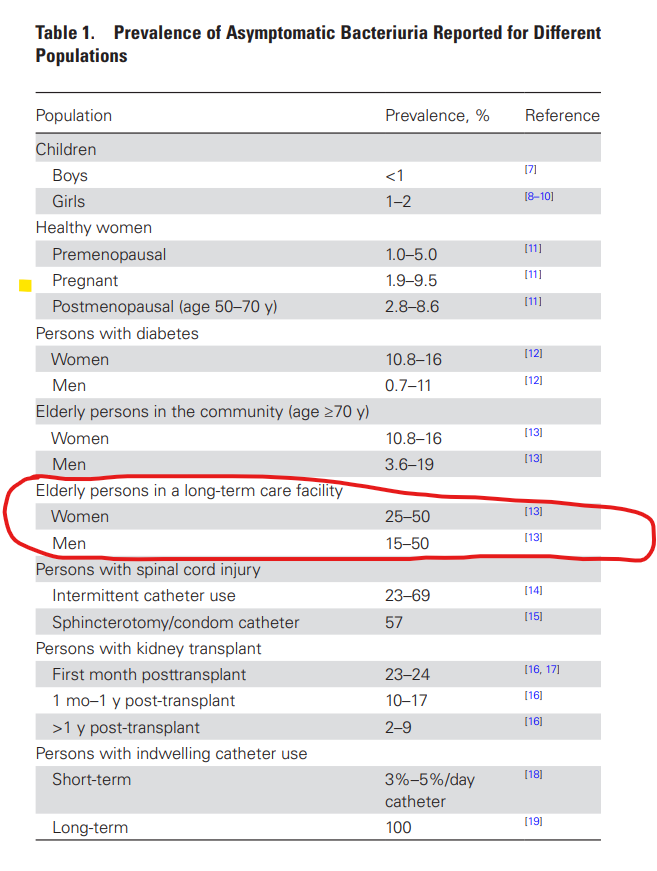
Asymptomatic bacteriuria in older adults: the most fragile women are prone to long-term colonization | BMC Geriatrics | Full Text (biomedcentral.com)
Conclusion: Institutionalized women with incontinence have ABU prevalence rates of about 80% and are often persistent carriers. Such prevalence rates should be considered in clinical decision making as they devalue the meaning of a positive urine culture as a criterion to diagnose UTIs. Diagnostic strategies are urgently needed to avoid antibiotic overuse and to identify patients at risk to develop upper UTI.
Urine PCR
- Conclusion: Moderately strong evidence exists that molecular diagnostics demonstrate increased sensitivity in detecting urinary bacteria at the expense of poor specificity in controls. Additional data comparing patient symptoms and cure rates following antibiotic selection directed by molecular methods compared with culture are needed to elucidate their place in UTI care.
- Of asymptomatic healthy controls, 95% had positive molecular tests vs 23% who had positive urine cultures
- Conclusion: Given the 40% discordance rate, the detection of ABR genes alone may not provide reliable data to make informed clinical decisions in UTI management. However, when used in conjunction with susceptibility testing, ABR gene data can offer valuable clinical information for antibiotic stewardship.
Diagnosing UTIs with Urine PCR | Clinical Lab Products (clpmag.com)
- The Centers for Medicare and Medicaid Services (CMS) indicates there are currently no FDA cleared/approved7 uses for a urine PCR multiplexed panel as there is no peer-reviewed published literature that demonstrates improved patient outcomes. CMS requires urine PCR testing to include parallel testing using conventional culture-based detection for correlation of results.
- LCD – MolDX: Molecular Syndromic Panels for Infectious Disease Pathogen Identification Testing (L39038) (cms.gov)
UTI Prophylaxis
- The growing crisis of antibiotic resistance has led to a reintroduction of methenamine as a viable and efficacious nonantibiotic management strategy for UTI prevention. Methenamine is as effective in UTI prevention as prophylactic antibiotics with a low side effect burden in randomized, controlled trials. Despite over a century of use, no bacterial resistance mechanisms or increased carcinogenesis have been observed. Although methenamine is gaining ground for UTI prevention, future studies will need to evaluate its longitudinal effect on host microbiota, both in and outside the urinary tract, and long-term impacts of such changes on subsequent health and disease. Given a new appreciation of the collateral damage of repeated antibiotic use on human health, effective nonantibiotic therapies, such as methenamine, must be revisited as part of the armamentarium in UTI prevention.
References
- The Bladder is Not Sterile: an Update on the Urinary Microbiome – PMC (nih.gov)
- Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by IDSA (idsociety.org)
- HAI Surveillance Protocol for UTI Events for LTCF (cdc.gov)
Resources:
- Suspected-UTI-action-tool_FNL.pdf (telligenqiconnect.com)
- Antimicrobial Stewardship in Long-Term Care Facilities | Department of Public Health & Environment (colorado.gov)
- Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults | Clinical Infectious Diseases | Oxford Academic (oup.com)