CDPHE Citations
- #1 citation has been lack of NHSN reporting — 224 citations.
- 8 facilities flagged for not meeting required RN hours.
- IJ tags — 3 for abuse, 2 for non-pressure skin conditions, 3 for accidents, 1 for emergency preparedness, 1 for failure to follow up Pharmacy recs, 1 for food textures, 1 for sanitary food services, 1 life safety related to fire suppression system.
Virus and Vaccine Update:
- You can give Influenza, COVID, and RSV vaccines on the same day.
- Getting a Flu Vaccine and other Recommended Vaccines at the Same Time | CDC
Influenza Vaccines –
- 3 antigens: A: H3N2, A: H1N1, B: Victoria; Hard to predict how the flu season this year will be.
- > 65 y/o give high dose influenza vaccine.
- Plan for giving flu vaccines to residents in October or early November.
- Vaccinate staff in September.
RSV Vaccine Update –
- Recommended for all adults >= 75 y/o
- Alternate recommendation to give vaccine to those >60 if they are at increased risk for severe disease.
- 85% efficacy of vaccine.
- GSK’s AREXVY has been shown to provide protection for up to 2 years.
- Pfizer’s ABRYSVO has been shown to provide protection for up to 2 years.
- Moderna’s mRESVIA has been shown to provide protection for up to 1.5 years (or 19 months).
- Vaccines for Adults Ages 60 and Over | RSV | CDC
- RSV Vaccine Information Statement | CDC
Avian Influenza H5N1 –
- 10-39 known human cases in 20 states.
- Usually, mild dz lasting days to week.
- 15% of asymptomatic farm workers are carriers of H5N1. It is likely spreading between cows via contaminated milking equipment.
- If we see airborne transmission happen, there is concern that this may become a larger issue in humans.
- The human influenza H1N1 component of our current vaccine MIGHT provide some protection to Avian flu H5N1.
- Antibodies to the N1 component from current vaccines might help protect you.
- US Invests in Avian Flu Vaccine Candidates (medscape.com)
New pnemococcal Vaccine – Capvaxive (PCV-21) is a new vaccine that might be available later this fall. It will probably be another option similar to the one-time dose of PCV20. Still waiting on final approval by CDC but the ACIP has endorsed it as another option for those who are eligible for pneumococcal vaccine.
- Covers serotypes responsible for approximately 84% of invasive pneumococcal disease in adults 50 years of age and older
- In adults 50 years of age and older, CAPVAXIVE covers the serotypes responsible for approximately 84% of Invasive Pneumococcal Disease (IPD) cases, compared to approximately 52% covered by PCV20.
- In adults 65 years of age and older, CAPVAXIVE covers the serotypes responsible for approximately 85% of IPD cases, compared to approximately 51% covered by PCV20.
- New Pneumococcal Vaccine Approved (medscape.com)
COVID –
- We expect a new COVID-19 Vaccine to be available in September/October; COVID vaccine 24-25.
- Unsure what the definition of up to date will be in the future. May require a yearly vaccine to be considered up to date.
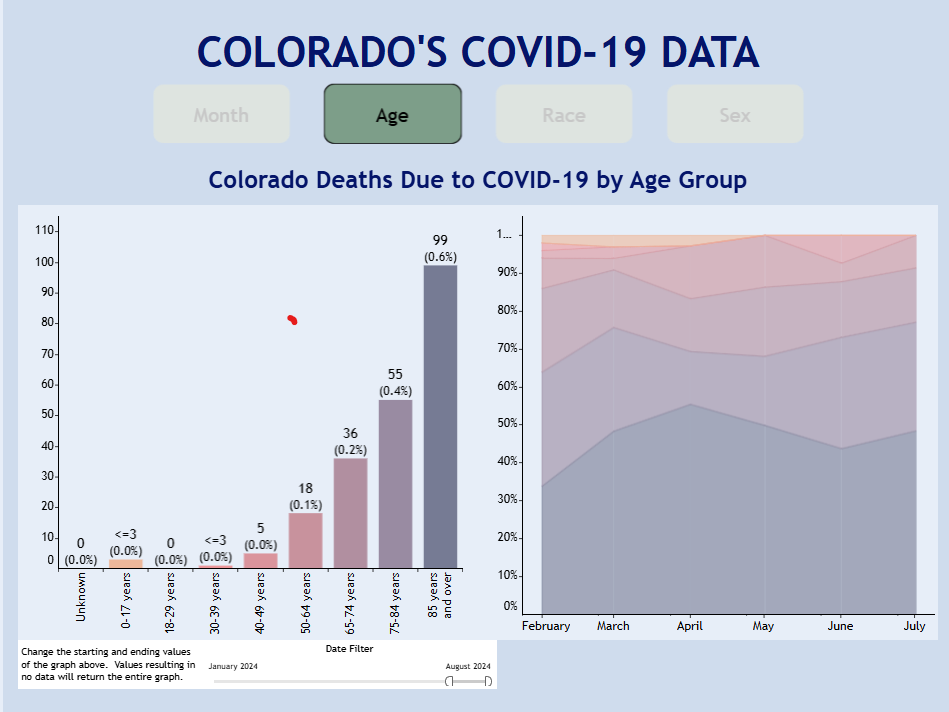
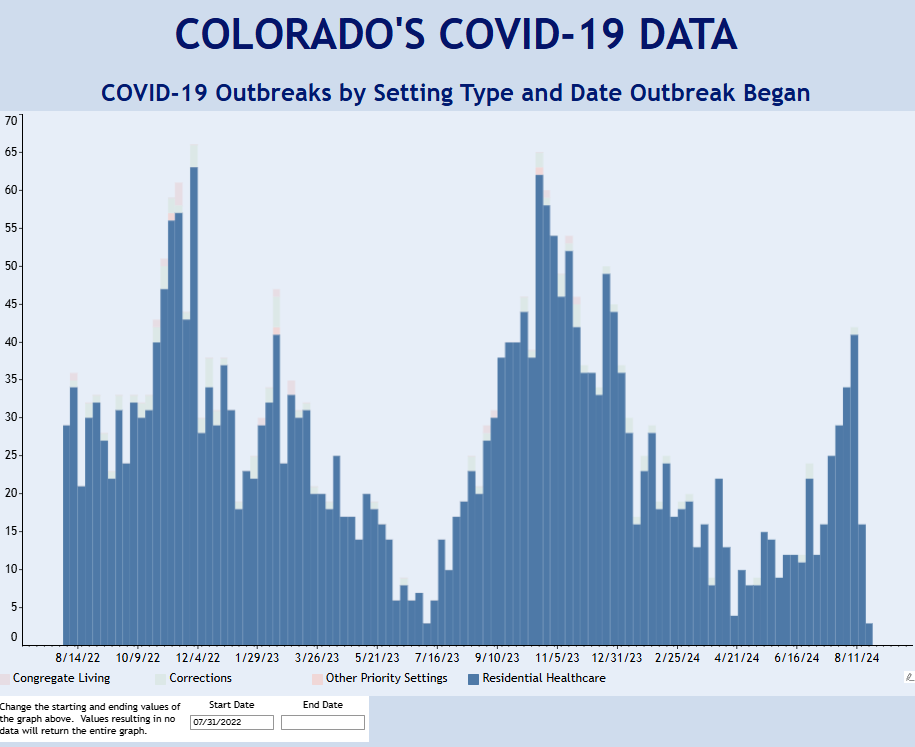
Residential Care Outbreaks
Staying Up to Date with COVID-19 Vaccines | COVID-19 | CDC
COVID-19 Data | Department of Public Health & Environment (colorado.gov)
Shingrix –
- two-dose series that can prevent shingles (herpes zoster) in adults
- recommended for those > 50 y/o
- 2 doses with the second dose given 2-6 months after the first dose
- Clinical trials show that the vaccine is more than 90% effective at preventing shingles and its complications, such as postherpetic neuralgia.
- Shingles Vaccination | Shingles (Herpes Zoster) | CDC
- Vaccine Information Statement | Shingles Recombinant | VIS | CDC
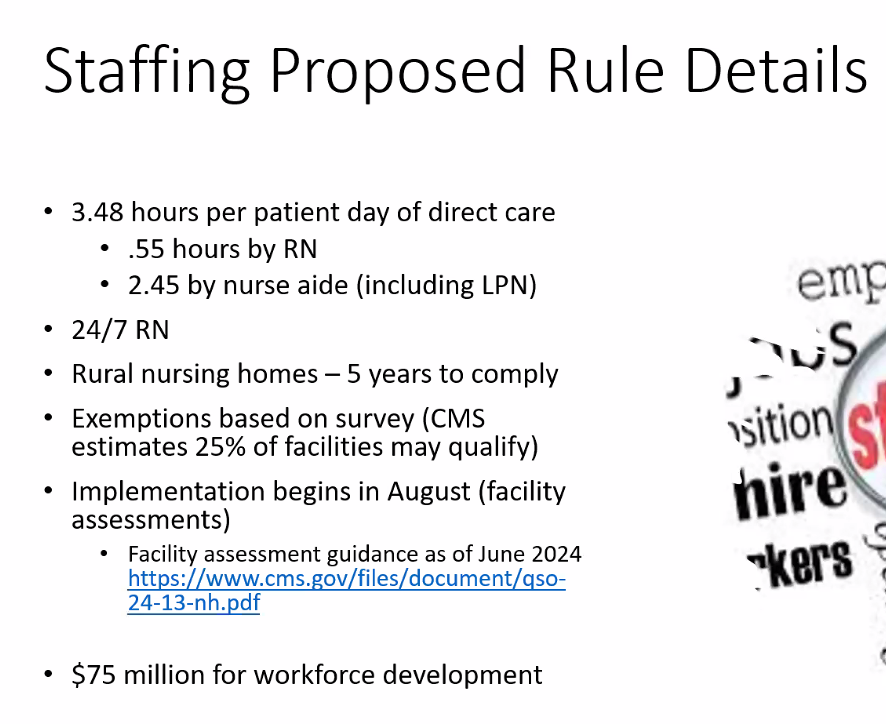
Revised Requirements for Facility Assessment
See revised requirements at this link –> Revised Guidance for Long-Term Care Facility Assessment Requirements QSO-24-13-NH (cms.gov)
excerpt from revised requirements…..
§ 483.71(b) In conducting the facility assessment, the facility must ensure:
§ 483.71(b)(1) Active involvement of the following participants in the process:
(i) Nursing home leadership and management, including but not limited to, a member of
the governing body, the medical director, an administrator, and the director of nursing;
and
(ii) Direct care staff, including but not limited to, RNs, LPNs/LVNs, NAs, and
representatives of the direct care staff, if applicable.
(iii) The facility must also solicit and consider input received from residents, resident
representatives, and family members.
§483.71(c) The facility must use this facility assessment to:
§483.71(c)(1) Inform staffing decisions to ensure that there are a sufficient number of staff
with the appropriate competencies and skill sets necessary to care for its residents’ needs as
identified through resident assessments and plans of care as required in § 483.35(a)(3).
§483.71(c)(2) Consider specific staffing needs for each resident unit in the facility and adjust
as necessary based on changes to its resident population.
§483.71(c)(3) Consider specific staffing needs for each shift, such as day, evening, night, and
adjust as necessary based on any changes to its resident population.
§483.71(c)(4) Develop and maintain a plan to maximize recruitment and retention of direct
care staff.
§483.71(c)(5) Inform contingency planning for events that do not require activation of the
facility’s emergency plan, but do have the potential to affect resident care, such as, but not
limited to, the availability of direct care nurse staffing or other resources needed for resident
care.
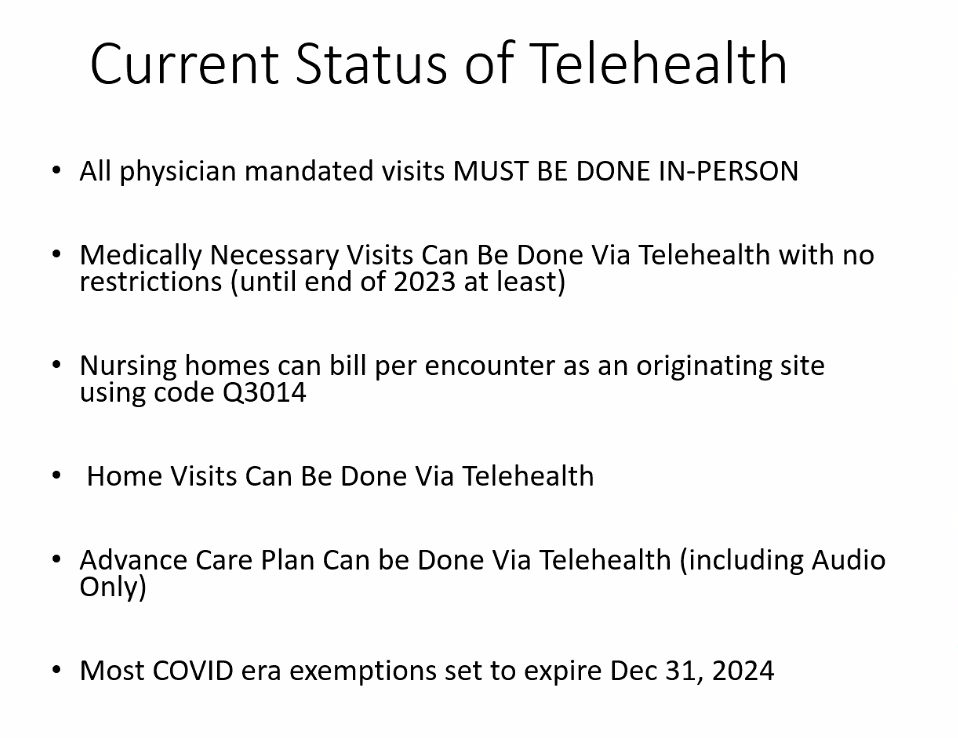
Telehealth in LTC