2022 AHA/ACC/HFSA Heart Failure Guideline: Key Perspectives – American College of Cardiology
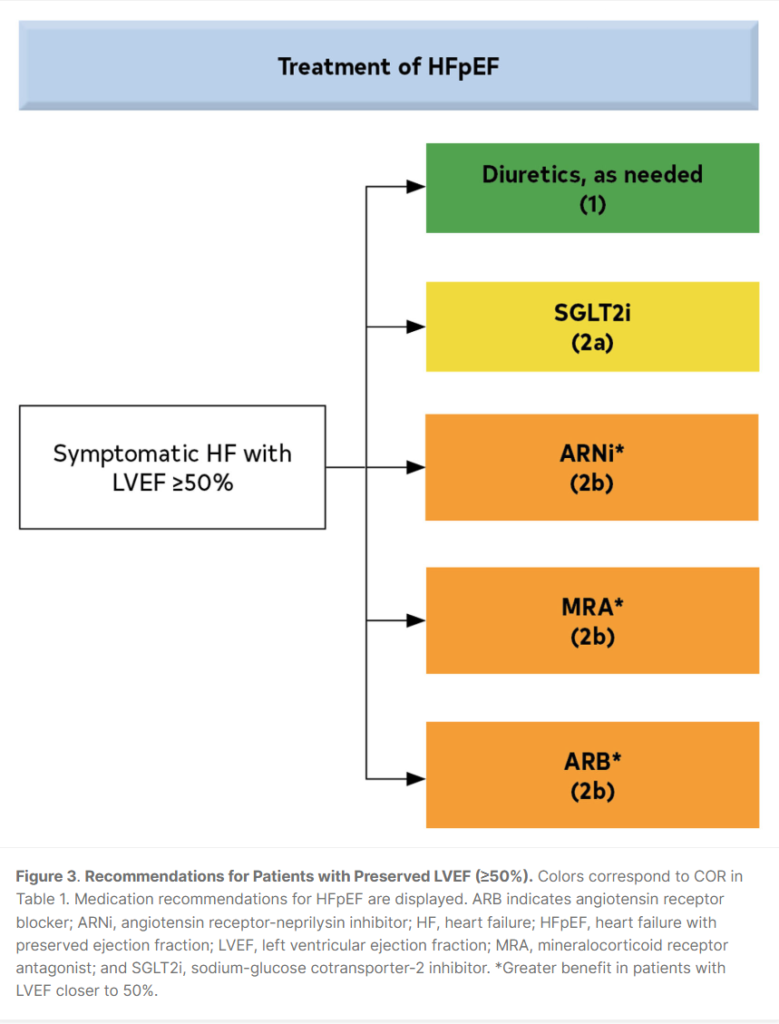
HFpEF LVEF > 50%
HFrEF LVEF <40%
Drugs:
- *** ARNi (Sacubitril/Losartan) / ARB / ACEi ***
- Beta blocker
- Mineralocorticoid receptor antagonists
- *** SGLT2i ***
- +/- Diuretics
#458 Heart Failure with Reduced Ejection Fraction – The Curbsiders
#460 Heart Failure with Preserved Ejection Fraction – The Curbsiders
The following are key perspectives from the 2022 American Heart Association (AHA)/American College of Cardiology (ACC)/Heart Failure Society of America (HFSA) Guideline for the Management of Heart Failure:
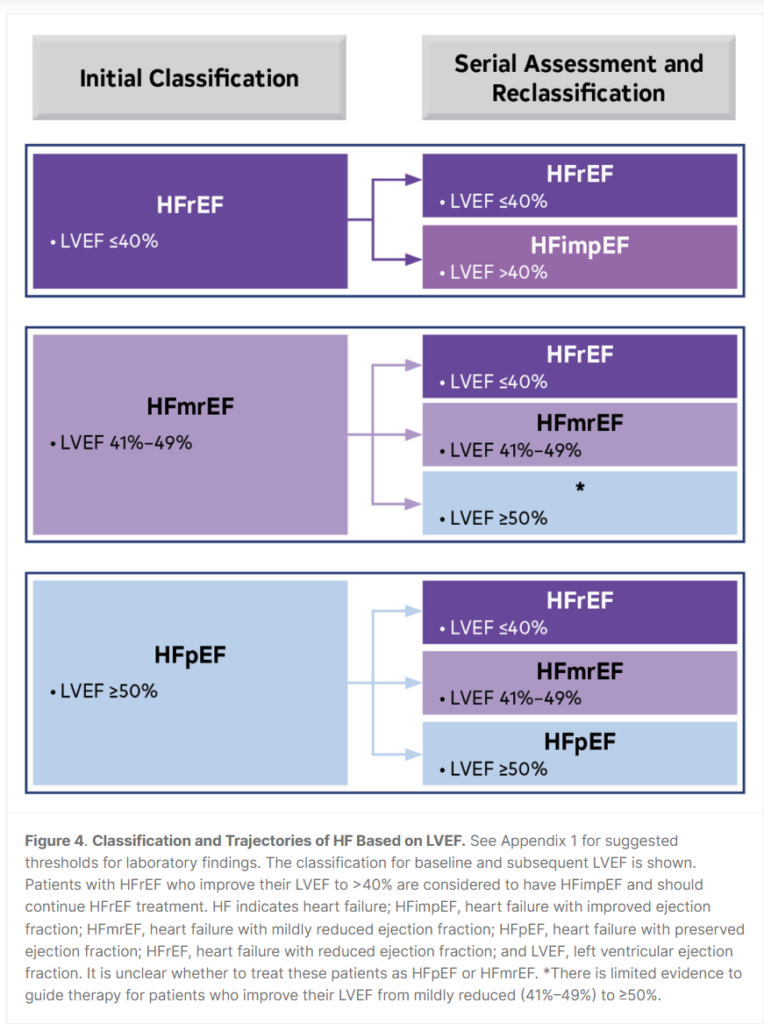
- Heart failure (HF) encompasses a broad range of left ventricular (LV) function. New treatment guidelines address the entire spectrum of HF. The classification of HF is as follows: HFrEF (HF with reduced ejection fraction [EF]): LVEF ≤40%; HFimpEF (HF with improved EF): Previous LVEF ≤40% and follow-up measurement of LVEF >40%; HFmrEF (HF with mildly reduced EF): LVEF 41-49%; HFpEF (HF with preserved EF): LVEF ≥50%. All patients with current or prior HF, irrespective of EF, should be considered for guideline-directed medical therapy (GDMT).
- GDMT has expanded to include four classes: 1) renin-angiotensin system inhibition (RASi) with angiotensin receptor-neprilysin inhibitors (ARNi), angiotensin-converting enzyme inhibitors (ACEi), or angiotensin (II) receptor blockers (ARB) alone; 2) beta blockers; 3) mineralocorticoid receptor antagonists (MRA); and 4) sodium-glucose cotransporter-2 inhibitors (SGLT2i). ARNi is now recommended as first-line RASi to reduce morbidity and mortality in HFrEF (Class of Recommendation 1a). ACEi is recommended when ARNi is not feasible, and ARB in those who are ACEi intolerant and when ARNi is not feasible. In symptomatic patients with HFrEF who tolerate ACEi or ARB, replacement with ARNi is recommended for further reduction in morbidity and mortality.
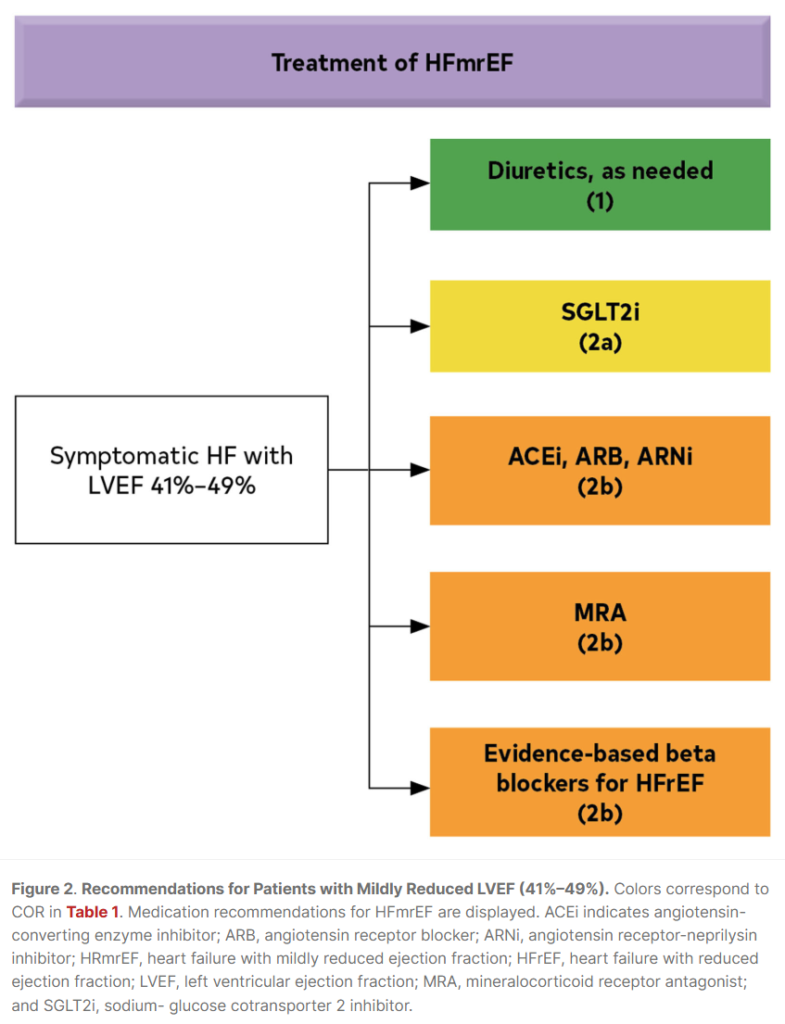
- New recommendations were made for the use of SGLT2i in HF. In symptomatic patients with chronic HFrEF, SGLT2i is recommended to reduce hospitalization and cardiovascular mortality, regardless of the presence of type 2 diabetes (Class of Recommendation 1a). SGLT2i can also be beneficial in patients with HFmrEF and HFpEF (Class of Recommendation 2a).
- While there is little data to guide management of patients with HFimpEF, a small, randomized trial (TRED-HF) demonstrated a high rate of relapse of dilated cardiomyopathy (44%) within 6 months of discontinuation of GDMT. Therefore, it is recommended that GDMT be continued in patients with HFimpEF, including those who are asymptomatic, to prevent relapse of HF and LV dysfunction.
- High value therapies (<$60,000/quality-adjusted life year gained) include ARNi, ACEi, ARB, beta blocker, MRA, hydralazine and isosorbide dinitrate in African Americans, implantable cardioverter-defibrillator (ICD), and cardiac resynchronization therapy (CRT), while SGLT2i and cardiac transplantation are of intermediate value. Tafamadis for amyloid was identified as low value (>$180,000/quality-adjusted life year gained), while mechanical circulatory support and pulmonary pressure monitoring are of uncertain value.
- Patients with suspected amyloid should undergo screening for monoclonal light chains, and if negative, bone scintigraphy should be performed to confirm the presence of transthyretin amyloid. Genetic testing is recommended in patients with transthyretin amyloid to differentiate hereditary variant from wild type. Tafamadis is recommended in select patients with wild-type or variant transthyretin amyloid to reduce cardiovascular morbidity and mortality (Class of Recommendation 1a). Anticoagulation is reasonable in patients with cardiac amyloid and atrial fibrillation to reduce the risk of stroke (Class of Recommendation 2a).
- Signs and symptoms of HF can be nonspecific. Therefore, supporting evidence of increased filling pressures, either invasive (hemodynamics) or noninvasive (diastolic function on imaging, natriuretic peptide) are required for confirmation of diagnosis when the EF is >40%.
- Timely referral for HF specialty care is recommended for advanced HF patients (if in accordance with goals of care) to review HF management and to assess suitability for advanced HF therapies.
- HF is a progressive disease, as highlighted by the ACC/AHA Stages of HF A-D. New terminology incorporates the designations “at-risk” and “pre-HF”. Primary prevention of HF, through lifestyle modification, screening, and management of risk factors and comorbid conditions, is recommended for those at risk (Stage A) or pre-HF (Stage B).
- Management of comorbid conditions in patients with HF may be beneficial. The new guideline provides recommendations for select patients with HF and anemia, iron deficiency, hypertension, sleep disorders, type 2 diabetes, atrial fibrillation, coronary artery disease, and malignancy.
Take Home Messages from the Guidelines
Summary of 2022 AHA HF Guidelines
Complete 2022 AHA HF Guidelines
CardioNerds – Democratizing Cardiovascular Education