
Liquids
| Risk Level | IDDSI Level | Description | Typical Indication |
|---|---|---|---|
| Lowest | 0 – Thin | Water, coffee | Safe swallow on MBS/FEES |
| Mild risk | 1–2 – Slightly/Mildly Thick | Nectar consistency | Delayed swallow trigger |
| Moderate risk | 3 – Moderately Thick | Honey consistency | Aspiration on thin & nectar |
| Highest risk (oral feeding) | 4 – Extremely Thick | Pudding consistency | Aspiration across thinner liquids |
| Unsafe for PO | NPO | Tube feeding | Silent aspiration, poor airway protection |
Solids
| Risk Level | IDDSI Level | Description |
|---|---|---|
| Lowest | 7 – Regular | |
| Mild risk | 6 – Soft & Bite-Sized | |
| Moderate | 5 – Minced & Moist | |
| Higher | 4 – Pureed | |
| Severe | 3 – Liquidised | |
| Unsafe | NPO |
For post-stroke dysphagia with increasing aspiration risk, progression follows a step-down in texture safety (more restrictive as risk increases), and a step-up during recovery.
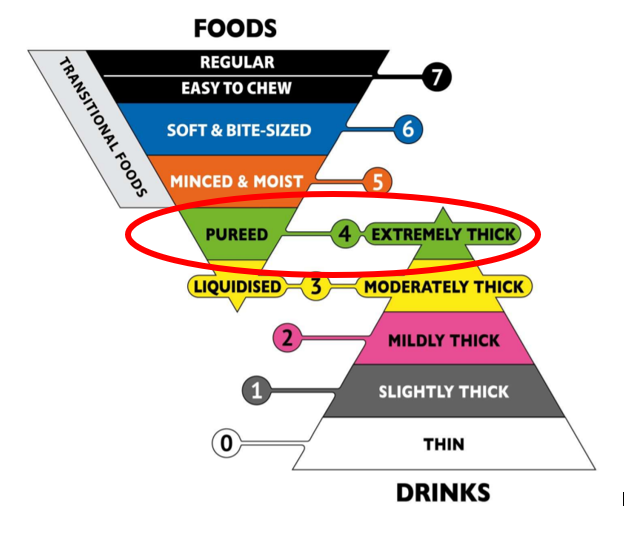
Using the International Dysphagia Diet Standardisation Initiative (IDDSI) levels:
1️⃣ Liquids – Typical Progression for Increasing Aspiration Risk
Thin liquids are highest risk in delayed swallow or poor airway protection.
🔽 Step-Down (as aspiration risk increases)
| Risk Level | IDDSI Level | Description | Typical Indication |
|---|---|---|---|
| Lowest | 0 – Thin | Water, coffee | Safe swallow on MBS/FEES |
| Mild risk | 1–2 – Slightly/Mildly Thick | Nectar consistency | Delayed swallow trigger |
| Moderate risk | 3 – Moderately Thick | Honey consistency | Aspiration on thin & nectar |
| Highest risk (oral feeding) | 4 – Extremely Thick | Pudding consistency | Aspiration across thinner liquids |
| Unsafe for PO | NPO | Tube feeding | Silent aspiration, poor airway protection |
Clinical Reality
Most stroke patients with aspiration start at:
- Level 2 (mildly thick)
or - Level 3 (moderately thick)
Level 4 liquids are used less commonly due to:
- Poor hydration tolerance
- Reduced patient acceptance
- Limited evidence of pneumonia reduction
2️⃣ Solids – Typical Progression
Solids generally move from least chewing demand to most as risk decreases.
🔽 Step-Down for Increasing Risk
| Risk Level | IDDSI Level | Description |
|---|---|---|
| Lowest | 7 – Regular | |
| Mild risk | 6 – Soft & Bite-Sized | |
| Moderate | 5 – Minced & Moist | |
| Higher | 4 – Pureed | |
| Severe | 3 – Liquidised | |
| Unsafe | NPO |
3️⃣ Most Common Post-Stroke Starting Points
In SNF/LTC stroke admissions with dysphagia:
- Pureed (Level 4) + Mildly/Moderately Thick liquids
is the most common initial order.
If silent aspiration or poor cough:
- Consider NPO with enteral feeding until reassessed.
4️⃣ Important Clinical Nuances (Where It Gets Subtle)
Liquids are more dangerous than solids
Thin liquids:
- Move quickly
- Require rapid swallow initiation
- More likely to be silently aspirated
Solids:
- Move slower
- Often easier to control if bolus prep intact
Thickened liquids are not benign
Risks:
- Dehydration
- Reduced intake
- Poor adherence
- Possible reduced medication absorption
Evidence does not show dramatic pneumonia reduction across all populations — so restriction should be proportional to risk.
5️⃣ Typical Recovery Progression (If Improving)
Example:
NPO
→ Level 4 puree + Level 3 liquids
→ Level 5 minced + Level 2 liquids
→ Level 6 soft + thin liquids
→ Regular
Advancement depends on:
- SLP reassessment
- Clinical signs (cough, wet voice)
- Instrumental study results
- Cognitive status
6️⃣ High-Risk Stroke Patterns
More restrictive textures are common in:
- Brainstem strokes
- Large hemispheric strokes with neglect
- Severe dysarthria
- Reduced level of consciousness