Pikes Peak Ethics Committee Meeting
- First Friday of every month at noon.
- Please consider bringing a case to the meeting. It’s a great opportunity to discuss difficult cases with your peers in LTC, share experiences, and learn from each other.
- Email me if you would like to be added to our email list to receive the agenda and reminders about the meeting.
- https://zoom.us/j/97461641616?pwd=YPpJU1ZHMG3bTChSVxAcD9gb39qVaY.1
World Elder Abuse Awareness Day

Observed Event on June 12th, 2026 in Colorado Springs, CO
Hosted by Pikes Peak Elder Justice Center
We invite you to partner with Pikes Peak Elder Justice Center as a sponsor of our
Fundraising Breakfast for World Elder Abuse Awareness Day. Your sponsorship supports
critical services for at-risk older adults in our community.
Sponsorship Levels:
Community Supporter – $250
Bronze Sponsor – $500
Silver Sponsor – $1,000
Gold Sponsor – $2,000
Presenting Sponsor – $3,000
Podiatry Orders
Standing orders for Podiatry services are under scrutiny from CMS. I think it is related to CMS’s concern about medical necessity for podiatry services. I would keep an eye on this as I suspect that we may start to see it more often. In general, if a patient needs a specialist, of any type (vision, podiatry, cardiology, wound care, PM&R), there should be a clear indication for the consultation. Generic standing orders for “podiatry to evaluate and treat” are becoming scrutinized. As far as utilization of healthcare resources, it probably makes sense that we have a clear indication for such consults.
- Podiatry consult – Diabetes, peripheral neuropathy, diabetes foot care and monitoring.
- Podiatry consult – PAD/PVD, high risk for foot wounds, PVD foot care and monitoring.
- Podiatry consult – Onychomycosis, high risk for foot wound, request Podiatry consult for difficult nail maintenance and treatment of chronic nail fungus.
Suicidal Safety Plan
- Please ensure that anyone that has a history of suicide attempts or active suicidal ideation has a suicide safety plan in place.
- Colorado Crisis Line dial 988
- Risk assessment tool – Columbia suicide Severity Rating Scale (C-SSRS) (screening version)
- Plan
- Means
- Intent
- Plan to act? When? Already started?
- Create a safety plan as though the person already has a plan.
- Make sure to use the words “thinking of killing yourself” when you assess the patient.
- Do not argue with a suicidal person and DO NOT try to convince them that they are fine.
- Lethality assessment
- Low Risk – Passive SI without plan and no intent
- q15 min checks, safety plan, regularly reassess risk, id coping skills
- Medium Risk – active SI with a plan but NO intent or past attempts with current passive SI.
- q15min checks,
- remove access to the means of committing suicide,
- 1:1 companion,
- safety plan,
- coping techniques,
- High Risk – active SI with a plan AND intent or past attempt with active SI with or without plan/intent.
- consider M1 Hold
- Usually 72 hrs but the evaluating doctor can cut that short if clinically justified
- Not to be used as a “just to be safe” measure
- consider M1 Hold
- Low Risk – Passive SI without plan and no intent
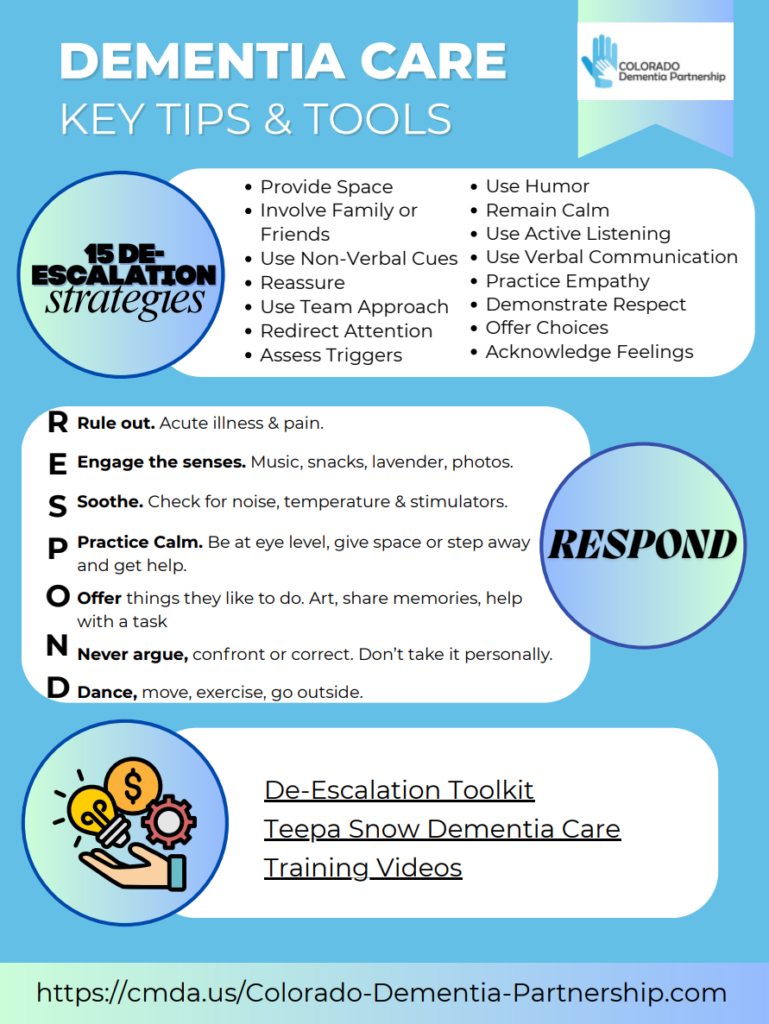
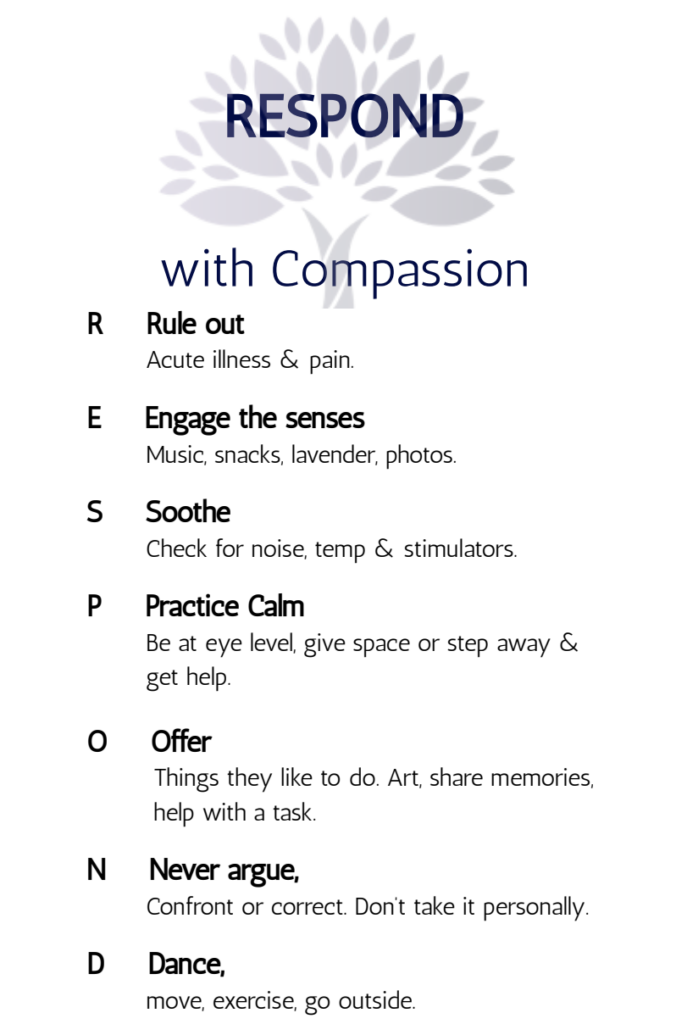
The Colorado Dementia Partnership
Fire Safety and Evacuation Plan
- Go over your facility fire safety requirements: firewalls, water, etc…
- Go over your plan for evacuation
- how are you getting meds out with patients?
- Organized plan for medications and oxygen? Throw them all in a bag and go?
- You may only have 20-30 minutes to get everyone out.
- Don’t count on pharmacy being able to send you new supplies of medications for all of your patients.
- how are you getting meds out with patients?
F841 — Medical Director
F841 is not about day-to-day patient care—it’s about system-level clinical leadership.
If care problems reflect system failure rather than individual physician error, surveyors often land on the medical director via F841.
Under F841, the facility must designate a medical director who is responsible for:
- Implementation of Resident Care Policies
- Ensures clinical policies are evidence-based and actually operationalized.
- Aligns physician services with facility protocols.
- Coordination of Medical Care
- Integrates attending physicians, NPs/PAs, nursing, pharmacy, and ancillary services.
- Reduces fragmentation (a common survey focus).
- Quality Assurance and Performance Improvement (QAPI) Involvement
- Active participation in QAPI.
- Drives improvement in outcomes (e.g., rehospitalizations, infections, antipsychotic use).
Anticoagulants and Anemia
We see a lot of people on eliquis/xarelto who also are on iron supplements for anemia. Please make sure we have appropriately worked up iron deficiency anemia. That would involve a stool hemoccult test to help rule out a lower GI bleed or colon cancer. It’s not perfect, but you can catch a lot of slow lower GI bleeds and colon cancer with this workup. I would also ensure that we check iron and hgb levels occasionally to assess efficacy of treatment if iron is continued.
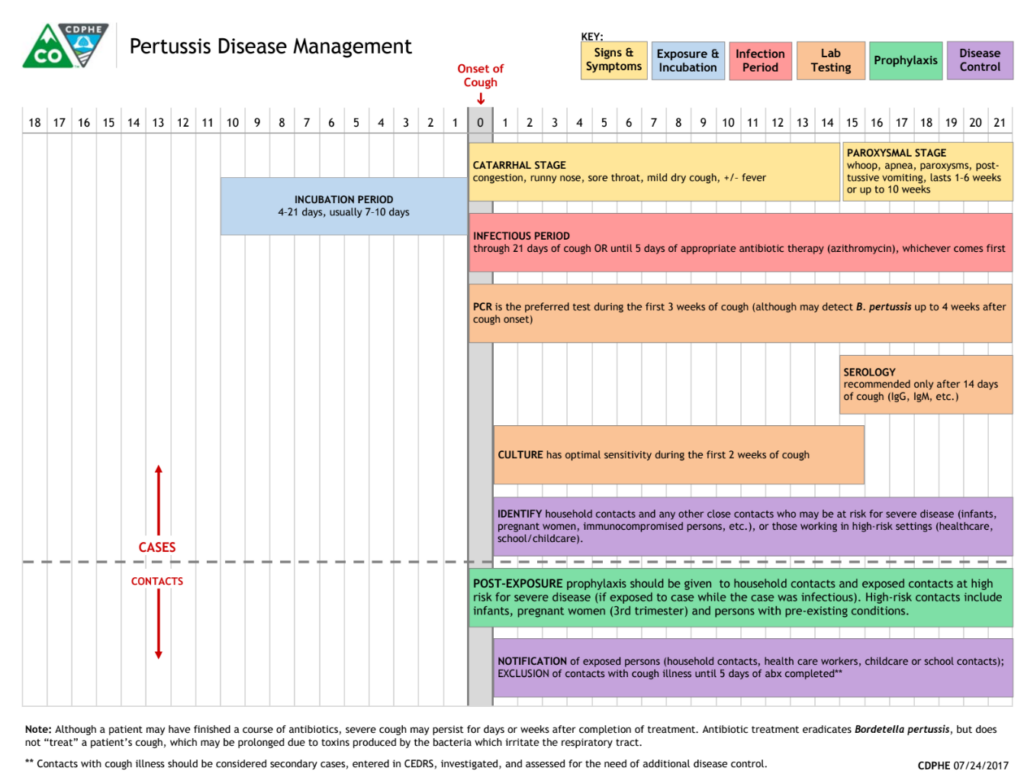
Pertussis (whooping cough)
There has been Pertussis activity in Colorado, in children primarily. There have been scenarios where a staff member’s child has pertussis. In this situation, the staff member should be seen by a physician, tested for Pertusis, and treated with prophylactic antibiotics (Azithromycin) BEFORE returning to work.
Facts to know:
Staff that have kids with Pertusis should be treated with azithromycin for 5 days, or alternative antibiotic, PRIOR to returning to work in LTC.
- Increased cases in Colorado since the COVID epidemic.
- Children are often affected first but adults and immunocompromised are at risk – nursing home residents.
- HIGHLY infectious.
- Antibiotic prophylaxis with azithromycin is often recommended for close contacts of cases.
- Incubation period is 5-21 days but most often presents at 7-10 days after exposure.
- A person is contagious for 21 days after coughing begins or until 5 days of antibiotic treatment has been completed.
Symptoms:
- Begins with mild cold symptoms (cough, congestion, runny nose) followed by intense coughing sessions that can last several weeks.
- Severe cough: It children is may end in a high-pitched “whoop” sound. This is not always true, especially in infants and adults.
- Hypoxia: Severe coughing fits may cause hypoxia.
- Vomiting: Coughing fits can lead to vomiting.
- Fatigue