
Prepare for Survey!! The focus will likely be on Infection Control, Life Safety, and Emergency Preparedness.
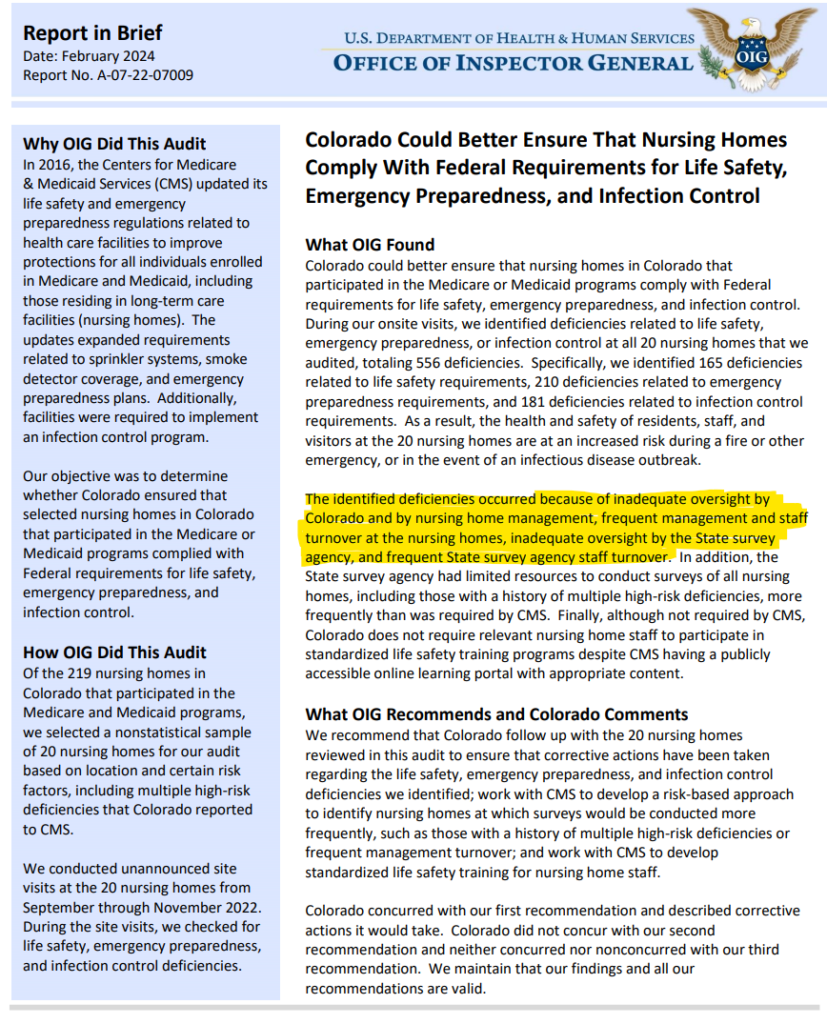
The Office of the Inspector General issued a report about Colorado nursing homes in February 2024. Full OIG report can be accessed at the link below. I encourage you to read this report paying special attention to the Findings section; there are pictures.
“The Findings detailed in our report show that nursing homes in Colorado, as well as their residents, could benefit from more frequent surveys. “
- Expect surveyors to focus on Infection Control, Life Safety, and Emergency Preparedness.
- Expect stricter enforcement and potentially more severe penalties for violations in these areas.
- I suspect that based on this OIG report, CDPHE will be pressured to FULLY enforce the CMS guidelines related to surveys/inspections and MAY prioritize who and how often to survey based on previous survey results (Risk-based strategy).
- CDPHE survey teams will likely increase the detail of ALL aspects of their investigations and inspections.
Keep Calm and Carry On: Managing Residents’ Anxiety While Managing Our Own
Let’s Consider a Scenario
A male resident has been observed to be agitated, short-tempered, and angry. He has been pacing the rehabilitation hall, tends to raise his voice at others, and is often seen watching the exit door. He has been choosing to not take his medications again for the third day in a row, and you observe an interaction between him and the medication aide.
The resident is sitting in the corner of his room, and the medication aide is insisting that he takes his medications. He begins to yell at her, calling her names and telling her to leave. She raises her voice to say, “I’m not leaving until you take your medications.” The resident responds by rising from his chair, seizing the medications, and throwing them across the room. The medication aide exits the room and tells her coworkers that she refuses to work with the resident again.
The resident is referred to a psychologist. His initial evaluation determined that he had smoked two packs of cigarettes per day before his admission, and he has been without nicotine for almost a week. He also is exhibiting moderate to severe anxiety symptoms and symptoms of PTSD related to combat exposure during the Korean War. He reports that he had been taking anxiety medication at home but has not been receiving it.
The medication aide in this scenario walked into the situation likely vulnerable to being triggered. She has a personal history of verbal abuse from her significant other and is frequently yelled at in her home life. She stayed to work an extra shift this day because the facility was short-staffed. She was also feeling pressure to hand out the medications quickly so she could leave soon to pick up her kids from school.
If we step back from this scenario, we can see that both the resident and the staff member brought predisposing factors into the interaction, which made both more susceptible to respond in an emotional manner at a stressful moment. Had the medication aide recognized that the resident’s agitation and anger could be anxiety related — that he was likely experiencing nicotine withdrawal, and that he has PTSD symptoms and may have felt cornered with his back against the wall — she could have used alternative responses. The medication aide, who feels stressed and emotionally triggered when yelled at, also could have politely stepped out and asked a coworker to assist in this potentially triggering situation.
Keep Calm and Carry On: Managing Residents’ Anxiety While Managing Our Own – Caring for the Ages
- Precipitating Events:
- Recent major medical diagnosis/terminal illness, surgery, or accident
- Significant change in medical status
- A new environment with strangers
- History of substance use
- Comorbid medical conditions
- Exposure to traumatic events
- Symptoms:
- Agitation, nervousness, irritability, or impatience
- A short temper
- Rapid breathing
- Verbalizing worrisome thoughts
- Restlessness
- Not wanting to leave their room
- Refusing therapies
- Avoiding interaction with others
- Difficulty concentrating
- Exaggerated startle response
- Insomnia
- Repeatedly asking to smoke
- Yelling/screaming
- Extreme focus on somatic issues
- Unprovoked physical aggression
Interventions:
- CALM: Your calmness can promote others to be calm as well.
- Music: For residents with dementia, research supports the use of playing music (Gerontologist 2019;59:e731–e742) to assist with managing anxiety symptoms. Music can lower heart rate, blood pressure, and other autonomic responses. Playing calming music could be beneficial for staff as well.
- Box Breathing: If Navy SEALs us it, it must work. Extending your exhalation trigger the parasympathetic nervous system which may lower heart rate and sympathetic drive.
- Inhale to a 4 count, hold breath for 4 seconds, exhale to a 6-10 count, hold for 4 seconds….repeat.
- Trigger: Is there a modifiable trigger to change or avoid?
- Exercise: Physical activity can help balance mood and calm the nervous system.
- Generalized Anxiety Disorder 7-item scale (GAD-7) — Printable copy of GAD 7
- PTSD Screen (PC-PTSD-5) — The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) (va.gov)
- Counseling
- Medications to treat Anxiety: First line – SSRI and SNRI.
- Psychiatry Evaluation
Mini Nutritional Assessment and Albumin
How to Try This: The Mini Nutritional Assessment : AJN The American Journal of Nursing (lww.com)
I have seen facilities utilize this Mini Nutritional Assessment as part of the admissions process. I found it a useful review and a tool that I refer to occasionally.
I would also remind you that the use of serum albumin for assessing nutritional status is not sensitive or specific as albumin can be affected by many disease states. It is a negative acute phase reactant…. inflammation (from many causes) reduces albumin/prealbumin.
- Many factors affect the albumin and prealbumin level.
- Normal prealbumin has been seen in studies of patients with BMIs as low as 12.9.
- Prealbumin is not always responsive to nutritional interventions.
- Changes in albumin/prealbumin do not always correlate with outcomes.
Summary Recommendation: Do NOT use Urine PCR testing. Stick to CBC, UA with C&S.
I have serious concerns that Urine PCR testing will lead to increased inappropriate use of antibiotics. If the physician/NP/PA does not understand the intricacies of the test, it is not unreasonable to expect that antibiotics may be prescribed when they are not needed, the wrong antibiotic may be prescribed, or an antibiotic with a broader than needed spectrum may be used. All of these cases increase the potential for antibiotic resistance and unnecessary antibiotic prescribing.
In general, PCR testing is VERY sensitive. It will pick up ANY bacteria that is in the sample. In urine, it will amplify contaminants, colonizers, as well as pathogenic organisms.
Urine PCR tests do NOT provide organism antibiotic sensitivities. The test identifies bacterial genes known to cause antibiotic resistance, but it does NOT provide clinically useful antibiotic sensitivities. The existence of a drug resistant gene in one single non-pathologic, contaminating organism could lead one to believe that a powerful broad-spectrum antibiotic is needed when in fact it is not.
The report will usually provide antibiotic recommendations based on genetic analysis (not sensitivities). I suspect that these recommendations are primarily aimed at ensuring that there is no liability taken on by the testing company. Thus, the recommendations are often for broader spectrum antibiotics than may be clinically necessary in order to limit medico-legal liability.
CDPHE did a pretty good presentation on Urine PCR Testing….see below.
Urine PCR Testing – docShepherd
Fun Facts:
Hyperkatifeia
the hypersensitive, negative emotional state associated with withdrawal from a drug. Opioid induced hyperalgesia might be an example. Increased anxiety during benzo withdrawal is another example.
Hyperkatifeia (derived from the Greek katifeia for dejection or negative emotional state) is defined as an increase in intensity of the constellation of negative emotional or motivational signs and symptoms of withdrawal from drugs of abuse. This overactive negative emotional state is also hypothesized to sensitize with repeated drug exposure and withdrawal and drive an increase in the role of negative reinforcement in maintaining substance use as addiction develops.
hyperkatifeia Optimized (youtube.com)
Addiction as a Coping Response: Hyperkatifeia, Deaths of Despair, and COVID-19 | American Journal of Psychiatry (psychiatryonline.org)
References
- Colorado Could Better Ensure That Nursing Homes Comply With Federal Requirements for Life Safety, Emergency Preparedness, and Infection Control (hhs.gov)
- How to Try This: The Mini Nutritional Assessment : AJN The American Journal of Nursing (lww.com)
- Stewardship strategies for interpretation of novel urinary diagnostics (docshepherd.com)
- Urine Polymerase Chain Reaction (PCR) Based Testing Guidance Document (wa.gov)
- Brief structured respiration practices enhance mood and reduce physiological arousal – PMC (nih.gov)
- A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7 | Anxiety Disorders | JAMA Internal Medicine | JAMA Network
- Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample – PMC (nih.gov)
- Addiction as a Coping Response: Hyperkatifeia, Deaths of Despair, and COVID-19 | American Journal of Psychiatry (psychiatryonline.org)
- Drug Addiction: Hyperkatifeia/Negative Reinforcement as a Framework for Medications Development – PMC (nih.gov)
- hyperkatifeia Optimized (youtube.com)
- Transition to drug addiction: a negative reinforcement model based on an allostatic decrease in reward function | Psychopharmacology (springer.com)