
Update from April CMDA call.
We need an informed consent for NEW psychotropic medications. We DO NOT need a new informed consent for changes in the dose of a medication that already has an informed consent.
COVID Vaccine Update
Special situation for people ages 65 years and older: People ages 65 years and older should receive 1 additional dose of any updated (2023–2024 Formula) COVID-19 vaccine (i.e., Moderna, Novavax, Pfizer-BioNTech) at least 4 months following the previous dose of updated (2023–2024 Formula) COVID-19 vaccine. For initial vaccination with updated (2023–2024 Formula) Novavax COVID-19 Vaccine, the 2-dose series should be completed before administration of the additional dose.
Clinical Guidance for COVID-19 Vaccination | CDC
Enhanced Barrier Precautions
Please Read: Frequently Asked Questions (FAQs) about Enhanced Barrier Precautions in Nursing Homes | HAI | CDC
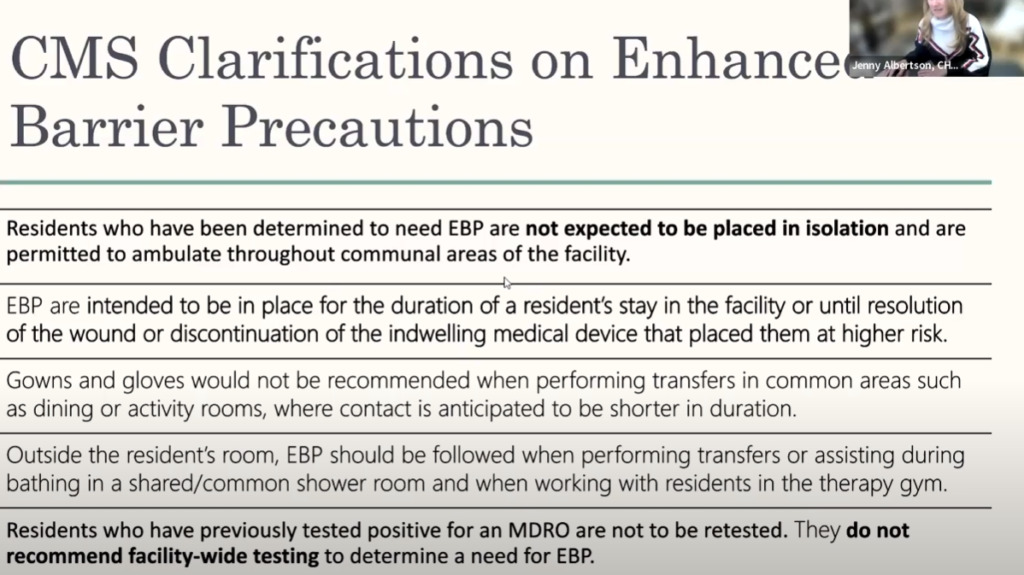
CDPHE surveyors are looking at EBP and how they are being implemented, QSO-24-08-NH. This is, generally, for high contact encounters where the staff will be interacting with a wound or indwelling device directly. I DO NOT recommend screening the entire facility. Approx 50% or more of LTC residents are colonized with an MDRO.
The new guidance is being incorporated into F880 Infection Prevention and Control, as or April 1, 2024.
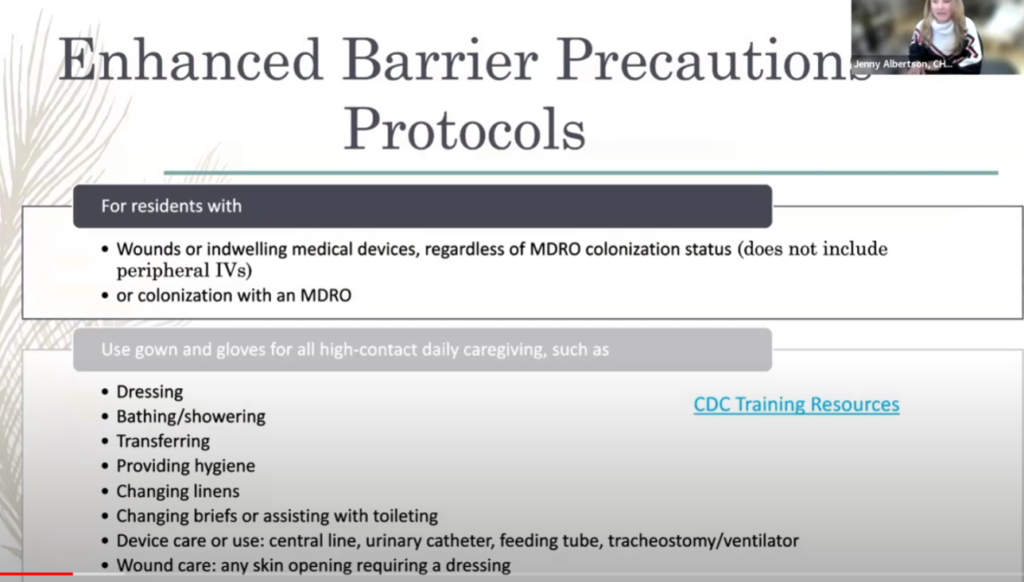
- Patients with wounds or indwelling medical devices regardless of MDRO colonization status. (excluding peripheral IVs)
- Patients with MDRO colonization.
Enhanced Barrier Precautions involve gown and glove use during high-contact resident care activities for residents known to be colonized or infected with a MDRO as well as those at increased risk of MDRO acquisition (e.g., residents with wounds or indwelling medical devices).
….
Enhanced Barrier Precautions expand the use of gown and gloves beyond anticipated blood and body fluid exposures. They focus on use of gown and gloves during high-contact resident care activities that have been demonstrated to result in transfer of MDROs to hands and clothing of healthcare personnel, even if blood and body fluid exposure is not anticipated. Enhanced Barrier Precautions are recommended for residents known to be colonized or infected with a MDRO as well as those at increased risk of MDRO acquisition (e.g., residents with wounds or indwelling medical devices). Standard Precautions still apply while using Enhanced Barrier Precautions. For example, if splashes and sprays are anticipated during the high-contact care activity, face protection should be used in addition to the gown and gloves.
Frequently Asked Questions (FAQs) about Enhanced Barrier Precautions in Nursing Homes | HAI | CDC
Examples of MDROs targeted by CDC include:
- Pan-resistant organisms,
- Carbapenemase-producing carbapenem-resistant Enterobacterales,
- Carbapenemase-producing carbapenem-resistant Pseudomonas,
- Carbapenemase-producing carbapenem-resistant Acinetobacter baumannii, and
- Candida auris
Additional epidemiologically important MDROs may include, but are not limited to:
- Methicillin-resistant Staphylococcus aureus (MRSA),
- ESBL-producing Enterobacterales,
- Vancomycin-resistant Enterococci (VRE),
- Multidrug-resistant Pseudomonas aeruginosa,
- Drug-resistant Streptococcus pneumoniae
Suicidal Ideation Across Long Term Care
Colorado Crisis Line dial 988
Risk assessment tool – Columbia suicide Severity Rating Scale (C-SSRS)
- Plan
- Means
- Intent
- Plan to act? When? Already started?
- Create a safety plan as though the person already has a plan.
Make sure to use the words “thinking of killing yourself” when you assess the patient.
Do not argue with a suicidal person and DO NOT try to convince them that they are fine.
- Lethality assessment
- Low Risk – Passive SI without plan and no intent
- q15 min checks, safety plan, regularly reassess risk, id coping skills
- Medium Risk – active SI with a plan but NO intent or past attempts with current passive SI.
- q15min checks,
- remove access to the means of committing suicide,
- 1:1 companion,
- safety plan,
- coping techniques,
- High Risk – active SI with a plan AND intent or past attempt with active SI with or without plan/intent.
- consider M1 Hold
- Usually 72 hrs but the evaluating doctor can cut that short if clinically justified
- If they do not fit the criteria, we cannot send them. Licensing boards are assessing the proper use of the M1 hold and reprimanding the improper use of this tool430 e.
- Not to be used as a “just to be safe” measure
- consider M1 Hold
- Low Risk – Passive SI without plan and no intent
References:
- Consideration for Use of Enhanced Barrier Precautions in Skilled Nursing Facilities HICPAC (cdc.gov)
- Frequently Asked Questions (FAQs) about Enhanced Barrier Precautions in Nursing Homes | HAI | CDC
- Enhanced Barrier Precautions in Nursing Homes (youtube.com)
- SUICIDAL BEHAVIOR (docshepherd.com)